Trauma, PTSD, Stress, Mental Health and Yoga
Trauma literally means a physical injury, or a deeply distressing, disturbing emotional event. Emotional or psychological trauma is often the result of a physical injury, or an overwhelming amount of stress that exceeds one’s ability to cope or integrate the emotions involved with that experience; it is the result of a real or perceived threat to life, or sexual violence. A traumatic event involves one experience, or repeating events with the sense of being overwhelmed that can be delayed by weeks, years, or even decades as the person struggles to cope with the immediate circumstances, eventually leading to serious, long-term negative consequences.
If the symptoms persist for more than one month, it is termed Post Traumatic Stress Disorder (PTSD). Most people having experienced a trauma event will not progress to PTSD. Assault-based trauma victims are more likely to develop PTSD. People who experience non-assault based trauma such as witnessing trauma, accidents, and fire events, are less likely to develop PTSD. Children, especially those less than 10 years of age, are less likely to experience PTSD after trauma. War veterans are more at risk for PTSD.
Trauma is a very common occurrence; according to an estimate, at least 1 in every 4 adults has suffered trauma at one or the other time in life. It is also one of the top five most costly health problems. This post discusses emotional or psychological trauma.
History
Trauma is as old as humans, although the diagnosis of post traumatic stress disorder or PTSD only made it into the Diagnostic and Statistical Manual of Mental Disorders (DSMV) in 1980. War, rape, natural disasters and abuse are as old as humans, and so is PTSD. Called soldier’s heart in the American Civil War, shell shock in the First World War, war neurosis in WWII, combat stress reaction in the Vietnam War, sometimes loosely labelled nervous breakdown, diagnosis that was gradually reformulated as PTSD.
There fell in this battle of Marathon, on the side of the barbarians, about six thousand and four hundred men; on that of the Athenians, one hundred and ninety-two. Such was the number of the slain on the one side and the other. A strange prodigy likewise happened at this fight. Epizelus, the son of Cuphagoras, an Athenian, was in the thick of the fray, and behaving himself as a brave man should, when suddenly he was stricken with blindness, without blow of sword or dart; and this blindness continued thenceforth during the whole of his after life. The following is the account which he himself, as I have heard, gave of the matter: he said that a gigantic warrior, with a huge beard, which shaded all his shield, stood over against him; but the ghostly semblance passed him by, and slew the man at his side. Such, as I understand, was the tale which Epizelus told.
– Herodotus (6.117 – Rawlinson translation)
The ancient Greek historian Herodotus describes that warrior Epizelus experiences hysterical blindness, possibly an extreme form of PTSD. The Greek playwright Sophocles has devoted Ajax and Philoctetes to devastating descriptions of the post-battle breakdowns. The hero Ajax kills hundreds of farm animals, believing them to be his commanding officers, and finally commits suicide by throwing himself on the point of his sword. “What should I do?” cries the despairing Ajax. “The gods hate me, the Trojans loathe me, the Greeks despise me!” The victims of PTSD are known to be at increased risk for homicide and suicide even today. Chaturanga (four limbs of the armed forces), or chatur, is an ancient two player Indian strategy game which is the common ancestor of the board games chess, shogi, makruk, xiangqi and janggi. Four player version was called chaturaji. It was described as shataranja by the Arab scholar Abu al-Hasan ‘Alī al-Mas’ūdī as a tool for military strategy, but also for reliving old battles, perhaps as a form of exposure therapy!
A brief recapitulation of history of PTSD is:
- 3000 BC (? 8000 B.C., or still older) – The horrendous combat events described in the Mahabharata and the demeanor and death of the main warrior characters such as Jayadratha graphically illustrate the trauma and symptoms now recognized as PTSD.
- 1900 BC – Egyptian physicians report hysterical reaction.
- 8 Century BC – Homer in The Odyssey describes flashbacks and survivor’s guilt.
- 730 BC – Homer’s great epic, The Iliad narrates a series of harrowing episodes of battle stress that were experienced by the ancient Hellenic combatants. He clearly paints the picture of the horror of war and trauma of combat. Achilles, the archetypal warrior, cries out in anguish and rage at the death and mutilation of his friend Patroklos.
- 490 BC – Herodotus writes of a soldier going blind after witnessing the death of a comrade next to him.
- 3 -5 BC – Jataka stories in Budhism
- 1597 – Shakespeare vividly describes war sequel in King Henry IV
- 1600 – Samuel Pepys describes symptoms in survivors of the great fire of London.
- 1879 – Rigler coins term Compensation Neurosis
- 1880’s – Pierre Janet studies and treats traumatic stress. He describes “hysterical and dissociative symptoms”, inability to integrate memories, by “phasic nature” of suppression and intrusion.
- 1899 – Helmut Oppenheim coins term Traumatic Neurosis
- WW-I : – “Shell Shock”
- WW-II : -“Battle fatigue”, “Combat exhaustion”, and, again, “Traumatic Neurosis”
- 1952 – Carl Jung analyses the psychological component of story of Job in Bible
- 1980 – PTSD becomes a diagnostic category in DSM
Careful research and documentation of PTSD began in earnest after the Vietnam War. The National Vietnam Veterans Readjustment Study estimated in 1988 that the prevalence of PTSD in that group was 15.2% and that 30% had experienced the disorder at some point since returning from Vietnam.
Cause
Stress, trauma or tension can happen due to many causes — a difficult or failed relationship, a financial hardship, a car accident, violence, an abuse, to name just a few. There is frequently a violation of the person’s familiar ideas about the world and of their human rights, putting the person in a state of extreme confusion and insecurity. This is also seen when a person feels violated or betrayed or disillusioned by some institution in unforeseen ways. Upsetting emotions, frightening memories, or a sense of constant danger may be the result. For most people, these symptoms are short-lived. They may last for several days or even weeks, but they gradually disappear.
But in some cases, the symptoms don’t decrease – one does not improve with each passing day. In fact, one may start to feel worse. The trauma may reflect in the body through the central nervous system. It may manifest as both emotional/ psychological as well as physical symptoms, ranging from flashbacks and anxiety, sensori-motor reactions as intrusive images, sounds, smells, body sensations, physical pain, constriction, numbing and even deep muscle patterns. These persisting trauma symptoms have the ability to derange one’s mental, psychological, biological, and social health.
An event will most likely lead to trauma if:
- it is unexpected,
- one is not prepared for it,
- feels unable to prevent it;
- happens repeatedly,
- someone is intentionally cruel, or,
- if it happened in childhood.
This can also be caused by one-time events, such as a horrible accident, a natural disaster, or a violent attack.
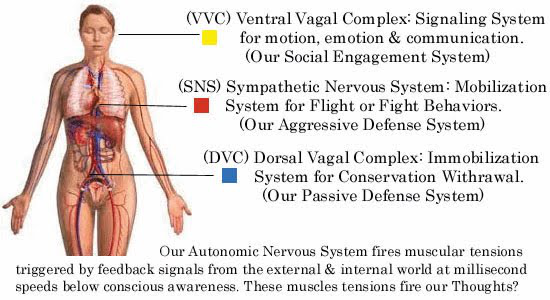
In case of a perceived or real threat, the first thing that happens is ‘sympathetic stimulation’, preparing the body for ‘fight or flight response. When the situation worsens further, in addition to changes in CNS, the ‘primitive dorsal vagus‘ elicits immobilization or ‘freeze‘ behavior; ventral vagus is connected with empathy, social communication and self-soothing behavior.
Neuroendocrinology of Trauma
PTSD symptoms may result when a traumatic event causes an over-reactive adrenaline response, which creates deep neurological patterns in the brain. These patterns can persist long after the event that triggered the fear, making an individual hyper-responsive to future fearful situations. During traumatic experiences the high levels of stress hormones secreted suppress hypothalamic activity that may be a major factor toward the development of PTSD.
The hypothalamic-pituitary-adrenal (HPA) axis is responsible for coordinating the hormonal response to stress. In PTSD, there is a maladaptive learning pathway to fear response through a hypersensitive, hyperreactive, and hyperresponsive HPA axis.
Low cortisol levels may predispose individuals to PTSD. People who suffer from PTSD have chronically low levels of serotonin, which contributes to the commonly associated behavioral symptoms such as anxiety, ruminations, irritability, aggression, suicidality and impulsivity. Serotonin also contributes to the stabilization of glucocorticoid production.
Low levels of dopamine can contribute to anhedonia, apathy, impaired attention, and motor deficits. Increased levels of dopamine can cause psychosis, agitation, and restlessness.
Hyperresponsiveness in the norepinephrine system can be caused by continued exposure to high stress. Overactivation of norepinephrine receptors in the prefrontal cortex can be connected to the flashbacks and nightmares. A decreased awareness of the current environment prevents the memory mechanisms in the brain from associating the flashback with the current environment.
Majority of reports indicate people with PTSD have elevated levels of corticotropin-releasing hormone, lower basal cortisol levels, and enhanced negative feedback suppression of the HPA axis by dexamethasone.
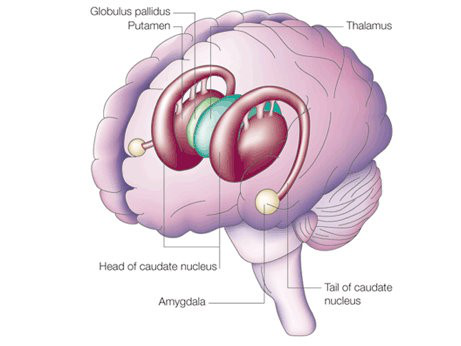
Neuro-anatomy of Trauma
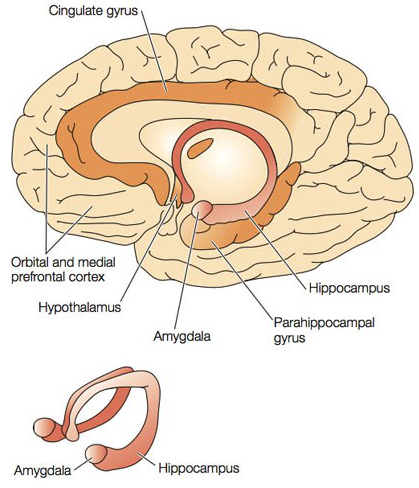
Three areas of the brain in which function may be altered in PTSD have been identified:
- prefrontal cortex,
- amygdala, and
- hippocampus.
PTSD is considered a syndrome of deficient extinction ability. The amygdala is a heterogeneous brain structure implicated in processing of emotions and storing the emotional aspects of memories. The amygdalocentric model of PTSD proposes that it is associated with hyperarousal of the amygdala and insufficient top-down control by the mPFC (medial prefrontal cortex) and the hippocampus in particular during extinction. Studies suggest that therapeutic strategies that enhance IGF2/IGFBP7 signalling and adult neurogenesis might be suitable to treat diseases linked to excessive fear memory such as PTSD.
Amygdala can also pre-empt neo-cortex through amygdala hijack; an amygdala hijack exhibits three signs: strong emotional reaction, sudden onset, and post-episode realization if the reaction was inappropriate.In human studies, the amygdala has been shown to be strongly involved in the formation of emotional memories, especially fear-related memories. During high stress times, the hippocampus, which is associated with the ability to place memories in the correct sequence and context of space and time, and with the ability to recall the memory, is suppressed. This suppression is hypothesized to be the cause of the flashbacks that often affect people with PTSD. When someone with PTSD undergoes stimuli similar to the traumatic event, the body perceives the event as occurring again because the memory was never properly recorded in the person’s memory.
The maintenance of the fear involved with PTSD has been shown to include the HPA axis, the locus coeruleus-noradrenergic systems, and the connections between the limbic system and frontal cortex. The HPA axis that coordinates the hormonal response to stress, which activates the LC-noradrenergic system, is implicated in the over-consolidation of memories that occurs as a result of trauma. This over-consolidation increases the likelihood of one’s developing PTSD. The amygdala is responsible for threat detection and the conditioned and unconditioned fear responses that are carried out as a response to a threat.
The LC-noradrenergic system has been hypothesized to mediate the over-consolidation of fear memory in PTSD. High levels of cortisol reduce noradrenergic activity, and because people with PTSD tend to have reduced levels of cortisol, it is proposed that individuals with PTSD fail to regulate the increased noradrenergic response to traumatic stress. It is thought that the intrusive memories and conditioned fear responses to associated triggers is a result of this response. Neuropeptide-Y has been reported to reduce the release of norepinephrine and has been demonstrated to have anxiolytic properties in animal models. Studies have shown people with PTSD demonstrate reduced levels of NPY, possibly indicating their increased anxiety levels.
The basolateral nucleus (BLA) of the amygdala is responsible for the comparison and development of associations between unconditioned and conditioned responses to stimuli, which results in the fear conditioning present in PTSD.
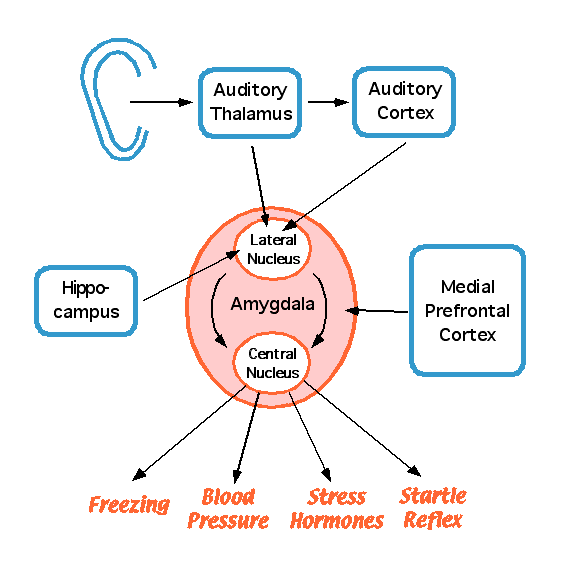
The BLA activates the central nucleus (CeA) of the amygdala, which elaborates the fear response, (including behavioral response to threat and elevated startle response). Descending inhibitory inputs from the medial prefrontal cortex (mPFC) regulate the transmission from the BLA to the CeA, which is hypothesized to play a role in the extinction of conditioned fear responses.
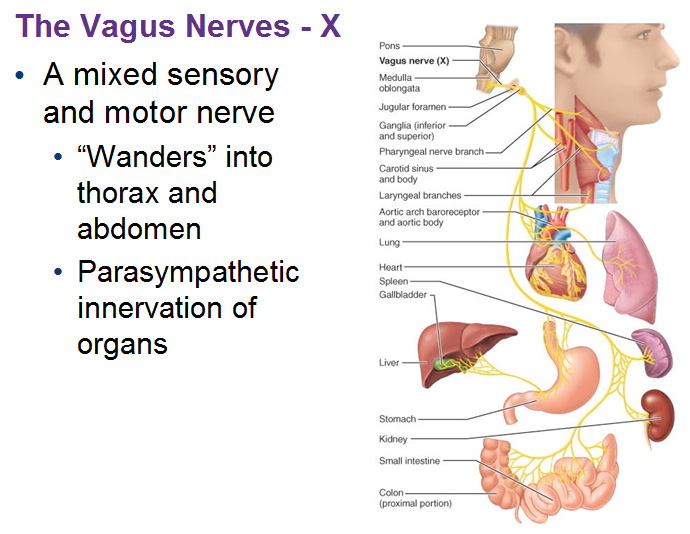
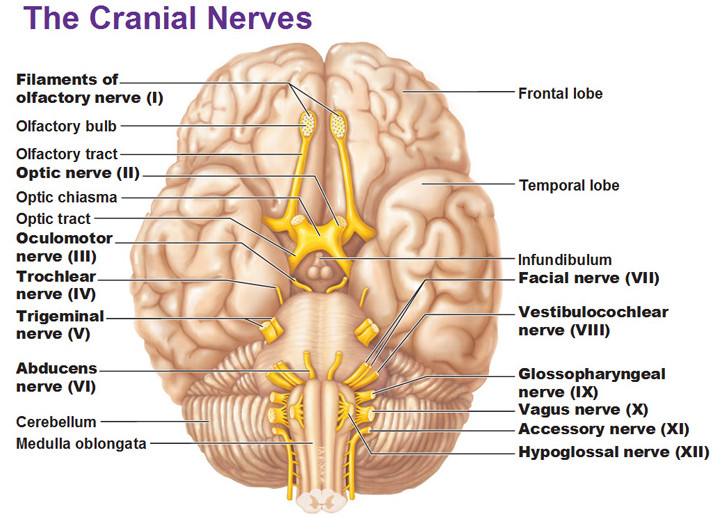
The Vagus Nerve
The vagus nerve (X cranial nerve) is a primary component of the autonomic nervous system. The word vagus means “wandering” in Latin. The words vagabond, vague, and vagrant come from the same root. The vagus nerve is known as the wandering nerve because it has multiple branches. This is one of the major nerves that goes to the brain. By stimulating the nerves, you can cause upstream changes in the brain without having to go into the brain.
Polyvagal theory outlines the structure and function of the two distinct branches of the vagus, both of which originate in the medulla. Each branch is associated with a different adaptive behavioral strategy, both of which are inhibitory in nature via the parasympathetic nervous system (PNS). The sympathetic-adrenal system is involved in mobilization behavior; vagus nerve acts opposite to this. According to polyvagal theory, these opposing systems are phylogenetically arranged.
Dorsal Vagal Complex (DVC)
The dorsal branch of the vagus originates in the dorsal motor nucleus and is considered the phylogenetically older branch. This branch is unmyelinated and exists in most vertebrates. Also known as the ‘vegetative vagus’, it is associated with primal survival strategies of primitive vertebrates, reptiles, and amphibians. Under great stress, these animals `freeze` when threatened, conserving their metabolic resources.
The dorsal vagal complex (DVC) provides primary control of sub-diaphragmatic visceral organs, such as the digestive tract. Under normal conditions, the DVC maintains regulation of these digestive processes. However, prolonged disinhibition can be lethal for mammals, as it results in apnea and bradycardia.
Ventral Vagal Complex (VVC)
A more sophisticated system with increased neural complexity evolved in mammals. This enriched behavioral and affective responses to an increasingly complex environment. The ventral branch of the vagus originates in the nucleus ambiguus and is myelinated to provide more control and speed in responding. It is also known as the “smart vagus” as it is associated with the regulation of sympathetic “fight or flight” behavior in the service of social affiliative behaviors. These behaviors include social communication and self-soothing and calming. In other words, this branch of the vagus can inhibit or disinhibit defensive limbic system, depending on the situation. The VVC provides primary control of supra-diaphragmatic visceral organs, such as the esophagus, bronchi, pharynx, larynx and heart. When vagal tone to the heart’s pacemaker is high, a baseline or resting heart rate is produced. In other words, the vagus acts as a restraint, or brake, limiting heart rate. However, when vagal tone is removed, there is little inhibition to the pacemaker, and so rapid mobilization (“fight/flight”) can be activated in times of stress, but without having to engage the sympathetic-adrenal system, as activation comes at a severe biological cost.
Vagal Tone
In order to maintain homeostasis, the central nervous system responds constantly, via neural feedback, to environmental cues. Stressful events disrupt the rhythmic structure of autonomic states, and subsequently, behaviors. Amplitude of respiratory sinus arrhythmia (RSA) is a good index of PNS activity via the cardiac vagus. That is, RSA is a measurable, noninvasive way to see how the vagus modulates heart rate activity in response to stress. This method is useful to measure individual differences in stress reactivity.
Research has shown that amplitude of RSA is an accurate indicator of the efferent influence of the vagus on the heart, and is widely used for this purpose. Since inhibitory effects of the VVC branch of the vagus allow for a wide range of adaptive, prosocial behaviors, it has been theorized that individuals with greater vagal tone are able to exhibit a greater range of such behaviors. On the other hand, decreased vagal tone is associated with illnesses and medical complications that compromise the CNS. These complications may reduce one’s capacity to respond to stress appropriately.
Chronic ‘freeze‘ reaction due to stress or unresolved trauma adversely impacts physical vitality and health:
- chronic tension patterns cause pain commonly in the neck/shoulder and lower back regions
- typical muscle patterns mainly in jaw, neck, throat, shoulders, diaphragm, pelvis and hamstrings
- adrenal fatigue occurs which in turn inhibits the immune system
- the ‘rest, digest and relax’ function of the Parasympathetic Nervous System never gets a chance to act
- digestive system is impaired; endocrine system is disrupted causing imbalance of growth hormones and reproductive hormones
- the body pH becomes acidic and promotes inflammation.
All of this leads to a variety of secondary illnesses including high blood pressure, cardiovascular disease, gastrointestinal problems, respiratory illnesses, immune disorders, to name just a few.
Trigeminal Nerve
The trigeminal nerve (V Cranial Nerve) is the fifth paired cranial nerve. It is also the largest cranial nerve. It is responsible for sensation in the face and motor functions such as biting and chewing. Its name derives from the fact that each trigeminal nerve (one on each side of the pons) has three major branches: the ophthalmic nerve , the maxillary nerve , and the mandibular nerve. The ophthalmic and maxillary nerves are purely sensory, and the mandibular nerve has sensory (or “cutaneous”) and motor functions. The trigeminal nerve originates from three sensory nuclei (mesencephalic, principal sensory, spinal nuclei of trigeminal nerve) and one motor nucleus(motor nucleus of the trigeminal nerve) extending from the midbrain to the medulla.
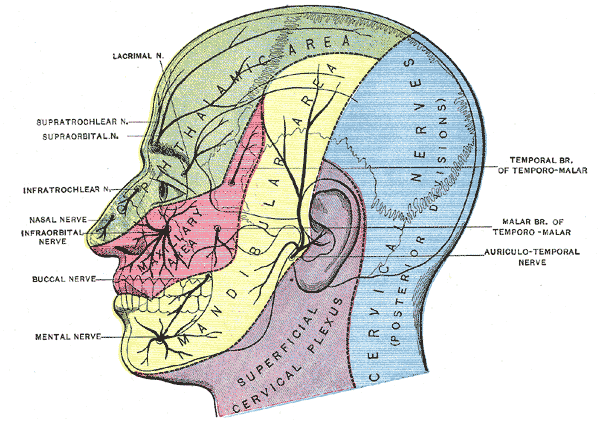
The ophthalmic, maxillary and mandibular branches leave the skull through three separate foramina:
- superior orbital fissure,
- foramen rotundum and
- foramen ovale.
The ophthalmic nerve carries sensory information from the scalp and forehead, the upper eyelid, the conjunctiva and cornea of the eye, the nose (including the tip of the nose, except alae nasi), the nasal mucosa, the frontal sinuses and parts of the meninges (the dura and blood vessels). The maxillary nerve carries sensory information from the lower eyelid and cheek, the nares and upper lip, the upper teeth and gums, the nasal mucosa, the palate and roof of the pharynx, the maxillary, ethmoid and sphenoid sinuses and parts of the meninges. The mandibular nerve carries sensory information from the lower lip, the lower teeth and gums, the chin and jaw (except the angle of the jaw, which is supplied by C2-C3), parts of the external ear and parts of the meninges. The mandibular nerve carries touch-position and pain-temperature sensations from the mouth. Although it does not carry taste sensation (the chorda tympani is responsible for taste), one of its branches—the lingual nerve—carries sensation from the tongue.
The two basic types of sensation are touch-position and pain-temperature. Touch-position input comes to attention immediately, but pain-temperature input reaches the level of consciousness after a delay. Touch-position information is generally carried by myelinated (fast-conducting) nerve fibers, and pain-temperature information by unmyelinated (slow-conducting) fibers. Touch-position and pain-temperature sensations are processed by different pathways in the central nervous system. This hard-wired distinction is maintained up to the cerebral cortex. Within the cerebral cortex, sensations are linked with other cortical areas.
The complex processing of pain-temperature information in the thalamus and cerebral cortex (as opposed to the relatively simple, straightforward processing of touch-position information) reflects a phylogenetically older, more primitive sensory system. The detailed information received from peripheral touch-position receptors is superimposed on a background of awareness, memory and emotions partially set by peripheral pain-temperature receptors.
As the trigeminal nerve has reciprocal projections to the nucleus tractus solitarius, the locus coeruleus, and the reticular formation, its role is implicated in mood regulation and anxiety disorders.
Pelvic Splanchnic Nerves
Pelvic splanchnic nerves or nervi erigentes are splanchnic nerves that arise from sacral spinal nerves S2, S3, S4 to provide parasympathetic innervation to the hindgut. The parasympathetic nervous system is referred to as the craniosacral outflow; the pelvic splanchnic nerves are the sacral component. They are in the same region as the sacral splanchnic nerves, which arise from the sympathetic trunk and provide sympathetic efferent fibers. They contribute to the innervation of the pelvic and genital organs. The nerves regulate the emptying of the urinary bladder, control opening and closing of the internal urethral sphincter, influence motility in the rectum as well as sexual functions like erection. They contain both preganglionic parasympathetic fibers as well as visceral afferent fibers. In the distal 1/3 of the transverse colon, and through the sigmoid and rectum, and the cervix in females, the pelvic splanchnic nerves supply parasympathetic function, including transmitting the sensation of pain. The proximal 2/3 of the transverse colon, and the rest of the proximal gastrointestinal tract is supplied its parasympathetic fibers by the vagus nerve.
Symptoms of trauma
Following trauma, people react in different ways, experiencing a wide range of physical and emotional reactions. Traumatic event is an ABNORMAL event and all reactions to it are NORMAL reactions.
Common physical symptoms of trauma can be: insomnia or nightmares, easy startling, racing heart, aches and pains, fatigue, difficulty concentrating, edginess and agitation, muscle tensions. Common emotional and psychological symptoms of trauma can be: shock, denial, or disbelief, anger, irritability, mood swings, guilt, shame, self-blame, feeling sad or hopeless, confusion, difficulty concentrating, anxiety and fear, withdrawing from others, feeling disconnected or numb. People who have lost a loved one may go through a grieving process. These symptoms may last from a few days to a few months, gradually fading as you process the trauma. But even when you’re feeling better, you may be troubled from time to time by painful reminders.
Diagnosis
Trauma, specifically Post Traumatic Stress Disorder (PTSD), is diagnosed based on signs and symptoms, a physical examination and a thorough psychological evaluation.
PTSD Mnemonic
E – Event/experience (threatening to life or physical integrity of self or others)
R – Re-experience (flashbacks, nightmares etc)
A – Arousal (anxiety, startling, hyper-vigilance, irritability)
A – Avoidance (of things, places, images etc. reminiscent of event)
D – Duration of more than one month
Criteria for PTSD are given in Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
DSM criteria for PTSD
Diagnosis of PTSD requires exposure to an event that involved or held the threat of death, violence or serious injury. Your exposure can happen in one or more of these ways:
- You experienced the traumatic event.
- You witnessed, in person, the traumatic event.
- You learned someone close to you experienced or was threatened by the traumatic event.
- You are repeatedly exposed to graphic details of traumatic events (for example, if you are a first responder to the scene of traumatic events).
You experience one or more of the following signs or symptoms after the traumatic event:
- You relive experiences of the traumatic event, such as having distressing images and memories.
- You have upsetting dreams about the traumatic event.
- You experience flashbacks as if you were experiencing the traumatic event again.
- You experience ongoing or severe emotional distress or physical symptoms if something reminds you of the traumatic event.
In addition, for more than one month after the traumatic event you may:
- Try to avoid situations or things that remind you of the traumatic event
- Not remember important parts of the traumatic event
- View yourself, others and the world in a negative way
- Lose interest in activities you used to enjoy and feel detached from family and friends
- Feel a sense of emotional numbness, feel irritable or have angry or violent outbursts
- Engage in dangerous or self-destructive behavior
- Feel as if you’re constantly on guard or alert for signs of danger and startle easily
- Have trouble sleeping or concentrating
Your symptoms cause significant distress in your life or interfere with your ability to go about your normal daily tasks.
For children younger than 6 years old, signs and symptoms may include:
- Reenacting the traumatic event or aspects of the traumatic event through play
- Frightening dreams that may or may not include aspects of the traumatic event
Seeking professional help
Everyone heals at his or her own pace and recovering from a traumatic event may take time. Professional help is indicated if even after months one is still experiencing symptoms.
One should seek professional help if one is:
- Suffering from great fear, anxiety, or depression
- Unable to form close, satisfying relationships
- Having trouble functioning normally at home or work
- Experiencing disturbing memories, nightmares, or flashbacks
- Trying to avoid more and more things that remind you of the trauma
- Feels emotionally numb and disconnected from others
- Using alcohol or drugs to feel better
Trauma treatment in Modern Medicine
Trauma freezes you in a state of fear and hyper-arousal and disrupts natural equilibrium. In PTSD, nervous system gets stuck in that traumatic state. Successful trauma treatment must re-establish your sense of safety and remove this imbalance.
Trauma treatment and healing entails:
- Discharging ‘fight-or-flight’ or ‘freeze’ emotions
- Processing trauma-related memories and feelings
- Learning how to regulate strong emotions
- Rebuilding the ability to trust other people
Different treatment options available in Modern Medicine are:
Psychotherapy
Several types of psychotherapy, also called talk therapy, may be used to treat children and adults with trauma. Some types of psychotherapy used in trauma treatment include:
Validation. Validation of the devastating impact of their initial trauma is the most healing thing. This relieves the burden of shame and guilt often associated with abuse.
Exposure therapy. This behavioral therapy helps you safely face what you find frightening so that you can learn to cope with it effectively. One approach to exposure therapy uses “virtual reality” programs that allow you to re-enter the setting in which you experienced trauma.
Somatic experiencing uses body’s unique ability to heal itself. This focuses on bodily sensations rather than thoughts and memories of the traumatic event; that gets you in touch with pent-up trauma-related energy and tension. Natural survival instincts take over from there, safely releasing this energy through various ways of expression like shaking, crying, and other forms of physical release.
EMDR (Eye Movement Desensitization and Reprocessing) is psychotherapy that emphasizes disturbing memories as the cause of psychopathology. This 8-phase therapy incorporates some elements of CBT with eye movements or other forms of rhythmic, left-right stimulation. These back-and-forth eye movements unfreeze traumatic memories, and resolve them.
Cognitive-behavioral therapy (CBT) helps you process and evaluate your thoughts and feelings about a trauma. Cognitive-behavioral therapy doesn’t treat the physiological effects of trauma; however, it can be helpful when used in addition to a body-based therapy such as somatic experiencing or EMDR.
Expressive therapy. Expressive therapies, expressive arts therapy or creative arts therapy, is the use of tactile, visual or other creative arts like Art Therapy, Music Therapy, Dance/ Movement Therapy, Drama Therapy, Poetry Therapy, Play Therapy, Sandplay Therapy, Multimodal Therapy etc as a form of therapy. The process of creation is emphasized rather than the final product. Expressive therapy can heal through use of imagination and the various forms of creative expression.
Medications. Most medications do not have enough evidence to support their use. Symptomatic medication – anti-anxiety, anti-depression, sedatives, may be prescribed for emotional trauma patients. Several types of medications can help improve symptoms of trauma:
- Antidepressants. These medications can help symptoms of depression and anxiety. They can also help improve sleep problems and concentration. The selective serotonin reuptake inhibitor (SSRI) medications sertraline (Zoloft) and paroxetine (Paxil) are approved by FDA.
- Anti-anxiety medications. These drugs also can improve feelings of anxiety and stress for a short time. Because these medications have the potential for abuse, they are not usually taken long term.
- Prazosin. If symptoms include insomnia or recurrent nightmares prazosin (Minipress) may help. It may reduce or suppress nightmares in many people with trauma.
Nerve Stimulators
Vagal Nerve Stimulator (VNS). Scientists have discovered that artificial Vagus Nerve Stimulation (VNS), through electrical impulses via a surgically implanted pacemaker like device, shows promising results in reducing depression, anxieties and even conditions such as epilepsy, obesity, PSTD, OCD(obsessive-compulsive disorder) and PD (Panic Disorder). VNS has also shown positive effects in promoting weight-loss as the signals to the brain of ‘fullness’ are more easily transmitted. The VNS device is sometimes referred to as a ‘pacemaker for the brain’. It is placed under the skin on the chest wall and a wire runs from it to the vagus nerve in the neck. VNS Therapy is designed to prevent seizures by sending regular, mild pulses of electrical energy to the brain via the vagus nerve. These pulses are supplied by a device something like a pacemaker. This is approved by FDA.
Trigeminal Nerve Stimulator (TNS). TNS can be delivered via the non-invasive external trigeminal nerve stimulation (eTNS) system or the minimally-invasive subcutaneous trigeminal nerve stimulation (sTNS) system for problems including epilepsy, depression, attention deficit hyperactivity disorder (ADHD), post-traumatic stress disorder (PTSD) Lennox-Gastaut syndrome (LGS), traumatic brain injury (TBI) and ADHD (attention-deficit/hyperactivity disorder). It works by sending signals in through the trigeminal nerve into the brain stem. From there, the signals can influence the activity in the centers of the brain that produce serotonin and norephinephrine, and also send signals to the anterior cingulate, the amygdala, the areas of the brain that are very important for things like emotional regulation and anxiety. This is still an investigational method.
Trauma self-help strategy
Break the cycle. When you feel anxious, take a brisk walk or jump into a hobby to re-focus.
Do not stay alone. Isolation makes things worse. Connecting to others will help you heal; so, make an effort to maintain your relationships and avoid spending too much time alone.
Support. Ask for the support if you need. Turn to a trusted family member, friend or a professional counselor.
Participate. Try to do normal things with other people that have nothing to do with the traumatic experience. Make the effort to reconnect.
Support group. Join a group of people with similar problems. Being with others who are facing the same problems can help reduce your sense of isolation, and hearing how others cope can help inspire you.
Volunteer. Volunteering can be a great way to challenge the sense of helplessness that often accompanies trauma. Remind yourself of your strengths and reclaim your sense of power by comforting or helping others.
Stay grounded. Have a structured schedule to follow. Stick to a daily routine, with regular times for waking, sleeping, eating, working, and exercise. Make sure to schedule time for relaxing and social activities, too. Break big tasks into smaller, manageable steps. Take pleasure from the accomplishment of achieving something, even it’s a small thing.
Find activities that make you feel better and keep your mind occupied (reading, taking a class, cooking, playing with your kids or pets), so you’re not dedicating all your energy and attention to focusing on the traumatic experience.
Allow yourself to express your feelings . Acknowledge your feelings about the trauma as they arise and accept them. Accepting your feelings is part of the grieving process and is necessary for healing.
You may want to go outdoors and find a peaceful place.
Take care of your health. A healthy body increases your ability to cope with stress from a trauma. Get plenty of sleep. After a traumatic experience, worry or fear may disturb your sleep patterns. A lack of sleep can make your trauma symptoms worse and make it harder to maintain your emotional balance. Go to sleep and get up at the same time each day and aim for 7 to 9 hours of sleep each night.
Avoid alcohol and drugs as their use can worsen your trauma symptoms and exacerbate feelings of depression, anxiety, and isolation.
Exercise regularly. Regular exercise boosts serotonin, endorphins, and other feel-good brain chemicals. It also boosts self-esteem and helps to improve sleep. For maximum results, aim for 30 to 60 minutes of activity on most days.
Eat a well-balanced diet. Eating small, well-balanced meals throughout the day will help you keep your energy up and minimize mood swings. While you may be drawn to sugary foods for the quick boost they provide, complex carbohydrates are a better choice. Foods rich in certain omega-3 fats—such as salmon, walnuts, soybeans, and flaxseeds—can give your mood a boost.
Reduce stress. Making time for rest and relaxation will help you bring your life back into balance. Try relaxation techniques such as meditation, yoga, or deep breathing exercises. Schedule time for activities that bring you joy—favorite hobbies or activities with friends, for example.
Helping someone in trauma
Helping a loved one who has suffered a traumatic or distressing experience may be tough, but your support can be a crucial factor in their recovery.
- Be patient and understanding. Healing from emotional or psychological trauma takes time. Don’t judge.
- Offer support to get back into a normal routine. That may mean help with collecting groceries or housework, for example, or simply being available to talk or listen.
- Don’t pressure your loved one into talking but be available when they want to talk.
- Help your loved one to socialize and relax. Encourage them to participate in physical exercise, seek out friends, and pursue hobbies and other activities that bring them pleasure. Take a fitness class together or set a regular lunch date with friends.
- Don’t take the trauma symptoms personally. Your loved one may become angry, irritable, withdrawn, or emotionally distant. This may be a result of the trauma and may not have anything to do with you or your relationship.
Helping a child
Following trauma, a child may show regression, tendency to take the blame, disturbed sleep or helplessness.
Regression. Many children may regress to an earlier stage, when they felt safer and more cared for. Younger children may wet the bed or want a bottle; older children may fear being alone. It’s important to be patient and comforting if your child responds this way.
Take the blame. Younger children tend to think that it must be their fault. Be sure the child understands that he did not cause the event.
Sleep disturbance. Some children have difficulty falling asleep, or wake frequently, or have troubling dreams. You can give your child a stuffed animal, soft blanket, or flashlight to take to bed. Try spending extra time together in the evening, doing quiet activities or reading. Be patient. It may take a while before your child can sleep through the night again.
Helplessness. Let them know that it’s normal to feel scared or upset. Your child may also look to you for cues on how they should respond to traumatic events so let him or her see you dealing with symptoms of trauma in a positive way.
Alternative Medicine
Yoga, including Meditation, can be a lifesaving healing technique for trauma and PTSD patients. Yoga helps by addressing deeply ingrained stress in the body and mind. By releasing held tension through yoga postures, breathing exercises, meditation practices etc, physical and emotional trauma stored even at autonomic level can be released. A somatic approach helps ease the feelings of helplessness, fear, arousal, and disconnection that can arise for trauma patients. Meditation acts at CNS level.
Tai Chi. Also called Chinese Yoga, this has benefits similar to Yoga.
Marma Therapy. Marma Therapy has a great vata calming effect. Marma points act through changes in blood flow and levels of neurotransmitters in the brain and spinal cord. A good Marma Therapy plan can be very helpful.
Massage therapy. Yoga and Ayurvedic massages, based on Marma points, have wonderful relaxing and healing effect. Even western massages – deep tissue massage, or Swedish massage, can reduce your heart rate, relax your muscles, improve range of motion in your joints and increase production of your body’s natural painkillers. It often helps relieve stress and anxiety.
Homeopathy. Homeopaths claim amazing results in PTSD! In classical Homeopathy, treatment for chronic ailments is constitutional. For acute cases, especially in case of a holocaust or a natural disaster, using Genus Epidemicus may suffice. A few remedies will most likely be very frequently required for the majority of the population. In a case of a natural disaster, such as an earthquake or a hurricane, the majority of relatively healthy people are going to respond with the picture of a limited number of remedies, e.g., Arsenicum, Ignatia amara, Aconitum, Arnica, Stramonium etc. The response to the remedy is claimed to be very dramatic and satisfying to both the patient and the practitioner.
Prognosis
With proper therapy, prognosis for PTSD is good. It depends upon the severity and length of time a person has suffered from the disorder. Psychotherapy can change brain chemistry. There are significant risks to a person with PTSD if they do not receive treatment – they may stay in a hyper-aroused state, further damaging their brain. Irritability, anxiety, or numbness may interfere with their ability to love and to work. Suicide is also a risk with untreated PTSD.
Yoga and Ayurveda in Trauma, PTSD, Stress and Mental Health
PTSD fits the Ayurvedic understanding of vata invading majja dhatu and manovahasrotas (mind channels). After witnessing or experiencing the trauma, the individual develops a set of vata symptoms that include repeatedly re-experiencing the trauma. Hyperarousal is an important vata condition leading to disproportionate responses to stimuli, e.g., startling.
Watch for symptoms of vata ojo vyapat (invasion of vata into ojas), such as extreme fatigue, memory issues and reversal of the diurnal cycle (awake at night and sleeping during day). However, because the amygdala is involved with anger as well as fear, there may well be a strong pitta component or even pitta ojo vyapat. Appropriate diet and lifestyle suggestions should thus be individually tailored within the prakriti-vikriti paradigm. The usual triad of diet, lifestyle and herbal therapies form the mainstay of chikitsa; other treatment interventions include oil therapies and Vedic stress reduction techniques like yoga and meditation.
Less is more, this applies especially to PTSD clients. So, move slowly.
Panchakarma Therapy

Pre-purification Measures namely ‘snehan‘ and ‘swedan‘ are very useful to balance ‘Vata‘ and to loosen the toxins. Snehan is the herbalized oil massage. This oil is applied to the entire body with a particular type of massage. Swedan is sweating and is given immediately following the snehan. A herbal decoction may be added to the steam to further enhance effect. This also provides a deeply soothing and balancing effect to the entire nervous system. The motion of massage creates heat and friction which enhances circulation and helps cleanse.
Diet and Nutrition
Sattwik food is preferable. Rajasik food leads to more activity and tamasik food leads to an increase in greed, anger, etc. Most of vegetarian food is sattwik; you can start with decreasing the percentage of non-vegetarian food in your diet. Concept of xenohormesis also favors vegetarian diet.
PTSD patients should have:
- Vegetable juice and soup
- Carrot, cucumber, beetroot juice
- Cooked vegetables like squash, zucchini and pumpkin
- Spices like cumin, coriander, ginger, asafoetida, garlic, fennel and turmeric.
- Green salad with a dressing of lemon juice and a little salt
- Khichadi (recipe made by cooking rice and mung dal)
- Desi Ghee (clarified butter) or Olive Oil.
The following should be avoided:
- Eating hot, spicy and fried foods, sweets, foods like brinjal, cabbage, cauliflower, spinach, broccoli, okra and potatoes.
- Too much tea, coffee, alcohol, white sugar, chocolate, cocoa.
- Sleeping during the day and staying up late at night
- Too much worry, anxiety, fear, stress and grief.
Ayurvedic Herbs

Ashwagandha is always useful where there is vata in majja dhatu and is known to increase dopamine levels, mitigating the over-activation of the amygdala. Bacopa or Brahmi can be used to help regulate serotonin production and can be combined with other nervine and adaptogenic herbs. These should be taken under the guidance of an expert Ayurvedic physician. Some bhasmas, which are prepared on the principle of potentization, can also be used to strengthen ‘nerves’.
Marma Therapy and Yoga/ Ayurvedic Massages

Vata soothing oil therapies that are valuable in PTSD include abhyanga with dosha specific massage oil such as Vata Massage Oil and shirodhara using Shirodhara Oil which contains nervine herbs such as brahmi, Bhringaraj, Ashwagandha and skullcap. Shirodhara has been shown to help normalize serotonin and noradrenaline levels and reduce anxiety and is traditionally said to remove vata from majja dhatu. Sarvangadhara or pizhichil with sesame oil can also be used to calm vata and normalize majja dhatu. Also, specific Marma points can be used for achieving specific results.
Therapeutic Yoga in Trauma
Yoga has always had a lot to offer. I’ve always called it a science beyond nano-science! Yoga and Yoga-based practices (YBP’s) have sparked new activity in new scientific research and one sees evidence of so much new research coming out of study of YBP’s – newer theories, newer bodily mechanisms, newer approaches to therapy, newer explanations! Yoga-based interventions have been associated with measureable changes in physiological parameters, perceived emotional states, and cognitive functioning. The scientific community should be careful and diligent in placing the credit of all these newer finds where it actually belongs.
Effective treatment for PSTD is possible through Yoga Therapy and we offer world-class Yoga Therapy services at SAVY under Dr Jitender K Sahdev. The real route to PSTD recovery lies in non-drug approaches that act on nerves, brain through asana, pranayama, meditation etc. And that points to the real solution. Lifestyle, and mind-body approaches that help with PSTD have something in common – they all help restore a balance of neurotransmitters in the brain and central nervous system. They are not just as effective as medication, but almost always safer and much less expensive. Efforts should be made to increase the Sattvic quality of mind.
Research indicates that a healthy vagus nerve is vital in experiencing empathy and fostering social bonding, and it is crucial to our ability to observe, perceive, and make complex decisions. Areas of distribution of trigeminal nerve and pelvic splanchnic nerves may also be utilized to achieve the same purpose. Tests have revealed that people with impaired vagal activity have also been diagnosed with depression, panic disorders, Post Traumatic Stress Disorder (PTSD), irritable bowel syndrome, anxiety, panic disorders, violent mood swings, fibromyalgia, early Alzheimer’s and obesity.
Through its array of asanas, drishti, pranayama, hasta, kaya, netra, adhaar mudras, bandhas, kriyas – neti, dhauti, nauli, basti, kapal bhati, and tratak, dhyana and more, with stimulation and healing effect on Vagus Nerve, Trigeminal Nerve, Pelvic Splanchnic Nerves, LHPA Axis, and even Neo-cortex, Yoga offers much less intrusive, non-invasive and natural way to maintain and regain health!
Asanas
Deep stretching is known to have a positive effect on PSTD. Some helpful poses are:
- Tadasana,
- Utkatasana
- Sarvangsamasana
- Halasana
- Viparitakarni,
- Bhujangasana,
- Virbhadrasana,
- Badha Konasana
- Setubandhasana
- Shavasana or Yoga Nidra
More of Vata reducing routines will be helpful. Regular practice of different postures should be done. Progressive deep relaxation, i.e., shavasana (corpse pose) brings about relaxation. At SAVY, we offer specialized TRY (SAVY Trauma Release Yoga) program specifically designed for PSTD.
Pranayama
According to Vedic scriptures, there is no disease which cannot be conquered through breath. Pranayama also creates a state of restful alertness in mind and body. Pranayama exercises like:
- Deergha Pranayama
- Visham Vritti Pranayama
- Mahat Pranayama
- Ujjayi,
- Bhastrika,
- Kapaal Bhaati,
- Anulom Vilom
are some of the exercises which can help in PSTD. All this must be undertaken strictly under proper guidance. Some clinical studies done in India have shown very positive results. Dr Sahdev’s Breathe and Heal Therapy, is one of the most effective and the safest breathing and mindfulness Yoga program specifically designed by a doctor for therapy.
Mudras
Hasta mudras attack the very root of problem; they address the issue of imbalance of five elements. Done for a minimum 45 minutes a day, they can be very effective.

These are some of the representative mudras:
- Gyan Mudra
- Vata-nashak Mudra
- Anjali Mudra
- Apana Mudra
- Apana-Vayu Mudra
- Prana Mudra
Shambhavi mudra, one kind of drishti, is very effective vagal stimulant. It should be learnt under an expert.
You should be able to notice the difference within a week. Mudras of the body, base, tongue, eyes etc form an integral part of our Yoga Therapy program. You can also join a specialized course on Hasta Mudras.
Meditation
Meditational therapies help the prefrontal cortex send calming messages to the amygdala. Both relative and absolute practices are important. Relative level practices may be more useful initially; relative practices include visualizations, affirmations, aspirations and relaxation practices. Visualizations work directly on the limbic brain and practices using words work on the prefrontal cortex. Visualization can include creating an image of a safe space and picturing oneself being there and relaxing. This sends messages of safety and relaxation to the limbic system. Affirmations can include positive phrases which help reprogram the prefrontal cortex to send healthy messages to the amygdala. Similarly, an aspiration practice can be used and combined with the breath. This practice helps the prefrontal cortex and limbic system to function normally. Once the mind is calmed by the use of relative practices, absolute practices such as vipashyana (mindfulness meditation) can be introduced. These practices help us see beyond the trauma by deepening our understanding of the impermanence of all phenomena. They have also been found to regulate prefrontal activity in favour of positive emotions.
Shatkarma
The six detoxifying procedures of Yoga:
- Neti,
- Dhauti,
- Nauli,
- Basti,
- Kapaal Bhaati, and
- Traatak
if done with proper technique, can be very helpful. Learn these under expert guidance at SAVY.
Lifestyle and Daily Routine
One of the most important factors is to have a lifestyle that does not disturb the natural body rhythm. When we eat, sleep and exercise in fluctuating and disturbing patterns, the body loses its natural cycle. Regularity in daily life can be extremely effective in reducing Vata imbalance. Expert Yoga Nutrition guidance is available at SAVY and should be availed.
TRY (SAVY Trauma Release Yoga)

SAVY offers this very effective and systematic approach for trauma, PTSD, stress and mental health. It teaches how to release deep chronic tension and stress, has immediate impact for most people, and can be integrated into a simple daily routine to help restore a sense of inner peace and emotional resilience. It is easy to learn and easy to practice. Benefits includes:
- Stress/Anxiety/Trauma/ Depression Relief
- Better emotional resilience
- Easing of neck/ shoulder/ low back pain or tension
These techniques induce healing at the deepest levels of body and mind.
Visit us at SAVY Studio for your individualized Therapeutic Yoga guidance and overall well-being.
You can book your appointment here.

If you have genuine interest in helping and empowering people with health issues, this program is especially for you!
Click on the image below to know details:
![]()
HEALING THROUGH BREATHING
NATURAL, SAFE, DRUG-FREE, EFFECTIVE
Note : DSBH Therapy ®, MBH Therapy® or TRY® has not been evaluated by Health Canada, US Food & Drug Administration or the American Medical Association. This technology does not claim to diagnose, treat, cure, or prevent any disease. Medical advice must only be obtained from a physician or qualified health practitioner. Results may vary between individuals. There are no guarantees, expressed, or implied.
You should check with your health care professional before starting this or any new therapy or exercise program or breathing routine. This is especially important if you have any pre-existing health conditions, such as high blood pressure, migraines or heart or lung ailments. Women who are pregnant or think they might be pregnant should consult their physician before performing any of the breathing or physical exercises or undertaking any therapy program.
The information contained in the program is not intended to serve as a replacement for professional medical advice. Any use of the information in these programs/ workshops is at the reader’s discretion, risk and responsibility. The studio, author and the publisher specifically disclaim any and all liability arising directly or indirectly from the use or application of any information contained herein. A health care professional should be consulted regarding your specific situation.
You must be logged in to post a comment.